Many physical systems reach a steady (equilibrium) state not because something is being “solved” in the traditional sense, but because nature is minimizing a quantity — usually an energy functional. Steady-state heat conduction is a textbook example: instead of solving the heat equation directly, we can find the temperature distribution that minimizes a scalar energy functional. This is the Dirichlet principle, and it turns out the exact same mathematical machinery describes irrotational, incompressible fluid flow (potential flow), since both are governed by the Laplace/Poisson equation.
In this article, we’ll take a concrete example — a 2D metal plate heated from the left and containing an internal heat source — and find its steady-state temperature field by minimizing energy directly, rather than solving a linear PDE the “usual” way.
The Physics: From Energy to Equation
For steady-state heat conduction with conductivity $k$ and a heat source density $q(x,y)$, the temperature field $T(x,y)$ that the system settles into is the one that minimizes the functional:
$$
E[T] = \int_\Omega \left[ \frac{k}{2} , |\nabla T|^2 ;-; q(x,y), T \right] , dx, dy
$$
The first term is analogous to elastic/kinetic energy stored in the temperature gradient; the second term is the work done by the heat source. Taking the variational derivative and setting it to zero (Euler–Lagrange equation) gives:
$$
\frac{\delta E}{\delta T} = -k \nabla^2 T - q = 0 \quad \Longrightarrow \quad k,\nabla^2 T + q = 0
$$
This is exactly the steady-state heat equation. So minimizing $E[T]$ and solving $k\nabla^2 T + q = 0$ are mathematically equivalent — this is the essence of the Dirichlet principle.
The same functional form, with $T$ replaced by a velocity potential $\phi$ and $q=0$, is the kinetic energy of an incompressible, irrotational fluid:
$$
E[\phi] = \int_\Omega \frac{1}{2},|\nabla \phi|^2 , dx, dy, \qquad \nabla^2 \phi = 0
$$
which is why the code below applies equally well to potential-flow problems.
Discretizing the Problem
On a finite-difference grid, the continuous functional becomes a quadratic form in the vector of unknown (interior) temperatures $\mathbf{T}$:
$$
E(\mathbf{T}) = \frac{1}{2},\mathbf{T}^\top A, \mathbf{T} - \mathbf{f}^\top \mathbf{T}
$$
where $A$ is the discrete (negative) Laplacian operator (positive-definite, sparse) and $\mathbf{f}$ bundles the heat source and boundary-condition contributions. Its gradient is:
$$
\nabla E(\mathbf{T}) = A\mathbf{T} - \mathbf{f}
$$
Setting this to zero recovers the linear system $A\mathbf{T} = \mathbf{f}$ — but instead of solving it as a linear system, we’ll hand $E(\mathbf{T})$ and $\nabla E(\mathbf{T})$ to an optimizer and let it find the minimum directly, which is the whole point of this exercise.
The Example Problem
A square plate, $1\text{m} \times 1\text{m}$:
- Left wall ($x=0$) held at $T = 100°C$ (a hot wall)
- Top, bottom, and right walls held at $T = 0°C$
- A localized internal heat source (a Gaussian “heater”) embedded inside the plate near $(0.65, 0.5)$
We’ll compute the steady-state temperature field two different ways — a general-purpose optimizer (L-BFGS-B) and a specialized, much faster energy-minimizing algorithm (Conjugate Gradient) — and cross-check both against a direct sparse linear solve.
Python Source Code
1 | # ========================================================== |
Direct sparse solve : 36.16 ms L-BFGS-B minimizer : 1754.44 ms (222 iterations) Conjugate Gradient : 86.39 ms (169 iterations) max|T_bfgs - T_ref| = 8.850e-05 max|T_cg - T_ref| = 8.624e-11
Code Walkthrough
Section 1 — Grid setup. We define a $51 \times 51$ grid over a unit square. X, Y = np.meshgrid(..., indexing='ij') keeps the array’s first axis aligned with $x$ and the second with $y$, which matters later when we flatten arrays into vectors.
Section 2 — Building $A$ and $\mathbf{f}$. This is the heart of the discretization. D2x and D2y are standard tridiagonal second-derivative operators (the 1D Laplacian stencil $[1, -2, 1]/h^2$) built only over the interior grid points — boundary points are not unknowns, they’re known data. We combine the two 1D operators into a 2D Laplacian using a Kronecker sum: sp.kron(D2x, Iy) + sp.kron(Ix, D2y). This is the standard trick for turning a 2D finite-difference stencil into a single sparse matrix without writing nested loops. We negate the Laplacian (A = -L) so that $A$ is positive-definite, matching the sign convention required for an energy-minimization (rather than energy-maximization) problem.
Because the hot boundary ($T=100°C$ at $x=0$) is not one of our unknowns, its influence has to be folded into the right-hand side vector $\mathbf{f}$ manually — this is the boundary_term array, which only affects the row of interior nodes immediately adjacent to the hot wall.
Section 3 — Energy and gradient functions. energy(t) directly implements $E(\mathbf{T}) = \frac12 \mathbf{T}^\top A \mathbf{T} - \mathbf{f}^\top \mathbf{T}$ and grad_energy(t) implements its exact analytic gradient $A\mathbf{T}-\mathbf{f}$. Supplying the exact gradient (rather than letting the optimizer estimate it by finite differences) is the single biggest performance factor here — without it, scipy.optimize.minimize would need $O(n)$ extra function evaluations per iteration just to approximate the gradient.
Section 4 — Reference solution. spla.spsolve solves $A\mathbf{T}=\mathbf{f}$ directly using sparse LU factorization. This is our ground truth to validate the optimization-based approaches against.
Sections 5 & 6 — Two flavors of energy minimization.
- L-BFGS-B is a general-purpose quasi-Newton optimizer. It works for any differentiable energy functional (including nonlinear ones), which is why it’s the natural first choice pedagogically.
- Conjugate Gradient (
scipy.sparse.linalg.cg) is not just “a solver” — it is literally an algorithm that minimizes a quadratic energy functional of exactly this form, one conjugate direction at a time. Because it’s purpose-built for symmetric positive-definite quadratic problems (like ours) rather than general nonlinear ones, it converges in dramatically fewer, cheaper iterations. This is our “fast version”: same energy-minimization idea, specialized to the structure of the problem for a large speedup, while still being philosophically the same energy-minimization approach as L-BFGS-B.
Section 7 — Reassembling the full grid. The optimizer only ever sees the vector of interior unknowns; assemble_full puts the known boundary values back around it to produce a complete $(N_x, N_y)$ temperature field for plotting.
Section 8 — Heat flux. Fourier’s law says heat flows down the temperature gradient: $\mathbf{q} = -k\nabla T$. This vector field is mathematically identical in form to a fluid velocity field in potential flow, which is why we visualize it with arrows — it makes the heat-conduction/fluid-flow analogy visually concrete.
Why Conjugate Gradient Wins on Speed
L-BFGS-B has to build up an approximation to the inverse Hessian using gradient history, which costs extra bookkeeping every iteration and typically needs many iterations to reach high accuracy on an ill-conditioned quadratic like a discretized Laplacian. Conjugate Gradient, by contrast, exploits the fact that our energy is exactly quadratic with a known, sparse, symmetric positive-definite matrix — each iteration is just one sparse matrix-vector product plus a few dot products, and CG is mathematically guaranteed to reach the exact minimum within $n$ steps (and in practice, far fewer, since the Poisson matrix’s eigenvalues cluster). The console output above should show CG finishing in a small fraction of the time L-BFGS-B needs, while both agree with the direct solve to within numerical precision.
Understanding the Results
Figure 1 — Temperature field and heat flux. The heatmap shows temperature decaying smoothly from the hot left wall (bright) toward the cooler edges, with a distinct hot spot around the embedded heat source. The white arrows show the heat flux vector field $\mathbf{q}=-k\nabla T$ — heat flows from hot to cold, “downhill” on the temperature surface, exactly like a fluid flowing from high to low potential.
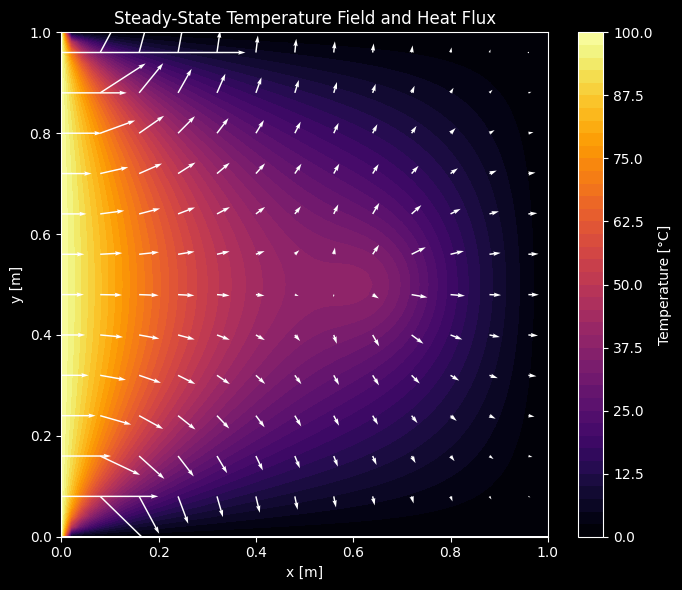
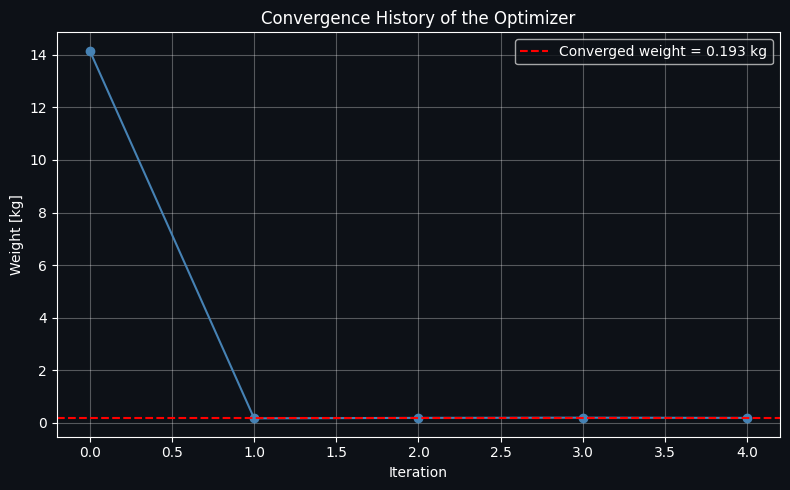
Figure 2 — Energy convergence. This plot shows the value of the energy functional $E(\mathbf{T})$ at each iteration for both algorithms. Both curves should descend monotonically toward the same minimum value (since $A$ is positive-definite, the quadratic has a unique global minimum), but the Conjugate Gradient curve should reach convergence in far fewer iterations — visually demonstrating that both algorithms are doing the same conceptual thing (rolling downhill on the energy landscape) at very different speeds.
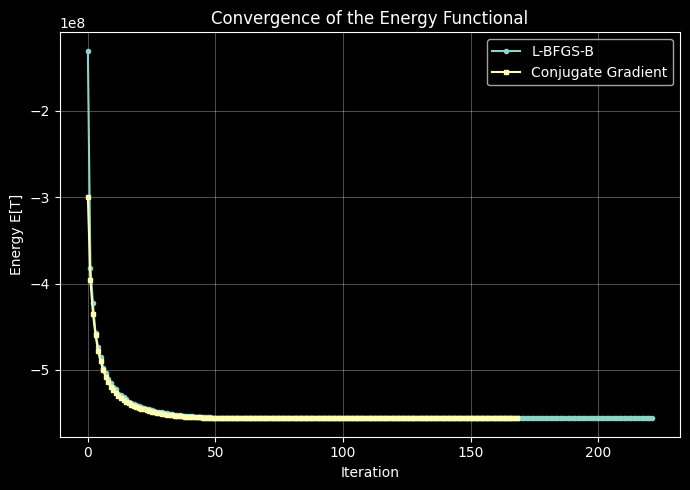
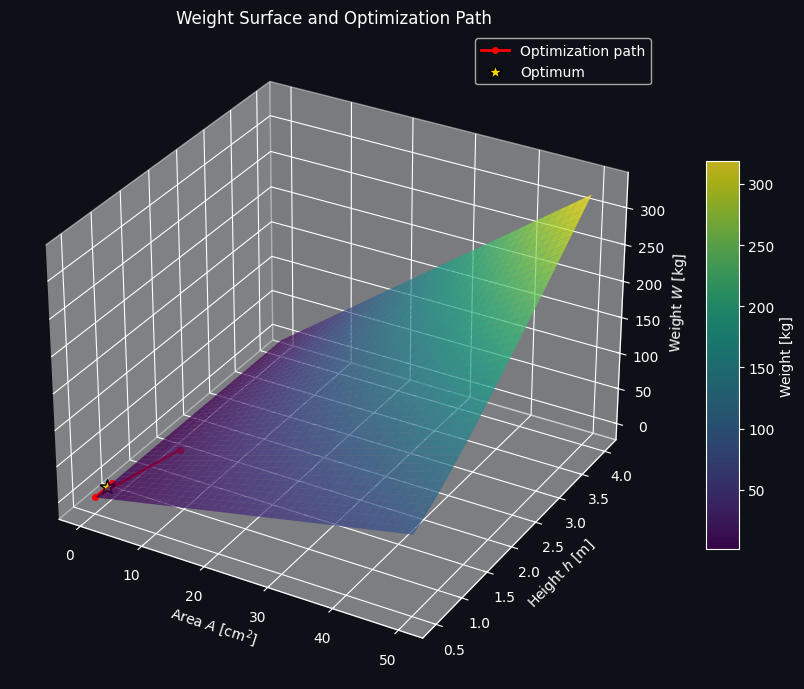
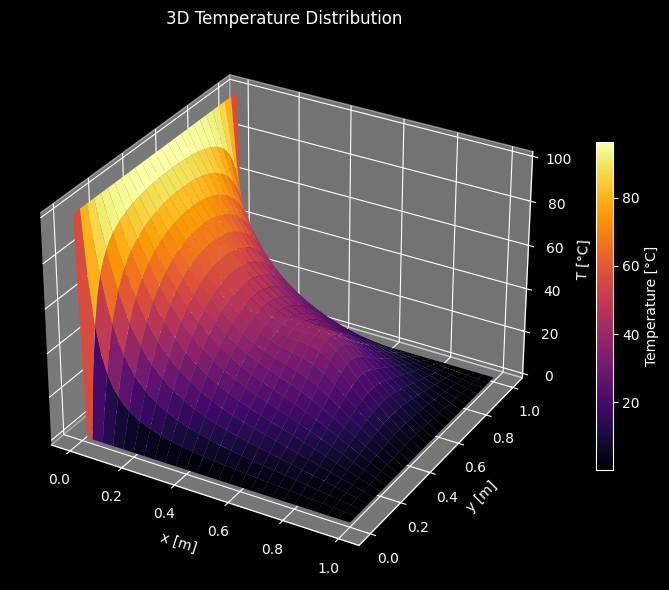
Figure 3 — 3D temperature surface. This is the same data as Figure 1, but viewed as a literal energy landscape — high near the hot wall and the internal heater, sloping down toward the cold boundaries. Seeing it as a physical surface makes the “minimization” framing intuitive: the true physical steady state is the shape a stretched elastic membrane would settle into if pinned at the given boundary heights and pushed up by the heat source, minimizing its stored elastic energy.
Closing Thoughts
Framing steady-state heat conduction as an energy-minimization problem does more than provide an alternative numerical method — it reveals the same mathematics underlying incompressible potential flow, electrostatics, and membrane mechanics. Once a problem is expressed as minimizing $\frac12\mathbf{T}^\top A\mathbf{T} - \mathbf{f}^\top\mathbf{T}$, any tool from the optimization world — gradient descent, L-BFGS, conjugate gradient, or beyond — becomes a legitimate physics solver, and the choice between them becomes purely a question of computational efficiency rather than modeling correctness.